
We have devoted a fairly substantial amount of attention to eating disorders on PBB. If you have read these articles or are familiar with eating disorders in general, you likely know that these diagnoses are significantly more common in women than they are in men. In fact, in anorexia nervosa (AN), more than 90% of those diagnosed are female. That being said, although they comprise only a small minority of individuals diagnosed with eating disorders, men nonetheless have been known to exhibit symptoms of disordered eating.
In the past, some researchers have focused primarily upon environmental causes of eating disorders and there is reason to believe that variables such as exposure to extremely thin celebrities in mass media can negatively influence eating behaviors (e.g., Iancu, Spivak, Ratzoni, Apter, & Weizman, 1994). Other researchers have focused primarily upon biological risk factors, with a particular focus on gonadal hormones as a potential explanation of the sex differences in eating disorders (Klump et al., 2006).
Today, I would like to discuss a study conducted by April Smith, Sean Hawkeswood, and Thomas Joiner of Florida State University that has been published in the International Journal of Eating Disorders but not yet been made available in print. In this study, the authors sought to examine the degree to which prenatal testosterone exposure - the amount of testosterone a fetus is exposed to while in the womb - predicted various facets of disordered eating in men. In this paper, the authors opened up with a discussion of the literature on the role of testosterone as an organizing hormone for men. Testosterone has been shown to play an important role in the masculinization of the human body and plays a vital role in the organization and development of several body parts, including genitalia, the brain, and other organ systems. Additionally, studies have demonstrated that higher levels of prenatal testosterone exposure predict cognitive abilities (e.g., mental rotation) and a variety of behavioral tendencies (Honekopp, bartholdt, Beier, & Liebert, 2007).
Importantly, prenatal testosterone exposure has also been directly linked to eating behavior. One study found that mice who received prenatal testosterone exposure consumed greater amounts of food and weighed more than mice who were not exposed to testosterone in utero (Donohoe & Stevens, 1983). In humans, studies have found that both female and male twins were less likely to exhibit eating disordered behaviors if they had been exposed to higher levels of prenatal testosterone (Culbert, Breedlove, Burt, & Klump, 2008). In that study, males from male-male twin pairs had less disordered eating than did males from male-female twin pairs and females from male-female twin pairs had less disordered eating than did females from female-female twin pairs. Because sharing a prenatal twin environment with a male twin is believed to increase prenatal testosterone exposure, the authors theorized that prenatal testosterone levels explained the findings.
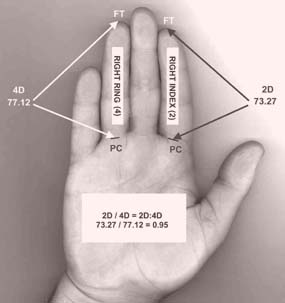
Smith, Hawkeswood and Joiner (in press) pointed out, however, that despite these promising findings, measuring prenatal testosterone levels is difficult and potentially dangerous, so alternative methods for obtaining this information are necessary. As it turns out, digit ratios - specifically, the ratio of the second finger to the fourth finger (2D:4D) - are strongly correlated with prenatal testosterone exposure, such that a lower ratio (longer fourth than second finger) is indicative of exposure to greater levels of prenatal testosterone. Men tend to have smaller 2D:4D ratios than women and research indicates that testosterone promotes the growth of the fourth finger whereas estrogen promotes the growth of the second finger (Honekopp et al., 2007). Now, if you are anything like me, you likely stopped reading halfway through this paragraph and looked to see what your ratio looks like. First of all, remember that you can not tell just from glancing how big or small your ratio is (although you can tell, to some extent, whether or not there is a difference between your second and fourth fingers). Additionally, remember that the research is not saying the individuals with a particular ratio are fated to particular outcomes, but rather that they are more vulnerable to those outcomes given the right environmental stress (or right environmental support, in the case of some of the more positive findings listed below).
Given all of these prior findings, Smith and colleagues (in press) wanted to determine whether a lower 2D:4D ratio - a sign of greater prenatal testosterone exposure - would predict lower levels of disordered eating in men. Additionally, because research has demonstrated that greater levels of prenatal testosterone exposure predict male physical fitness and athletic prowess, even when controlling for age, experience, and type of sport (Bailey & Hurd, 2005; Manning & Taylor, 2001), the authors wanted to see if a lower 2D:4D ratio would be associated with a lower drive for leanness and a greater drive for muscularity.
The sample of this study consisted of 204 undergraduate males, 78% of whom were Caucasian and 37% of whom reported being gay. Ages ranged from 17 to 24. To measure disordered eating, the authors used the eating disorders examination questionnaire (EDEQ-4). Importantly, to measure eating attitudes and drive for particular body type, the authors used a scale specifically designed for men - the male body attitudes scale (MBAS). The authors used the digit ratio from participants' left hands, as they found a significant difference between the ratio on the left and the right, with the left hand proving to be more "masculinized." Prior studies have reported similar findings (Luce & Crowther, 1999), leading to the assumption that the left hand provides the truer estimate of prenatal testosterone exposure (although this is not a universally accepted belief).
Results from this study were, in large part, consistent with the authors' hypotheses. Drive for thinness was lower in men with a lower 2D:4D ratio and drive for muscularity was higher in men with a lower 2D:4D ratio. In other words, the greater the level of prenatal testosterone exposure, the less likely a male was to feel driven to be lean and the more likely he was to feel driven to have a muscular physique. Both of these relationships remained significant when gay men were included in the analyses. Additionally, both relationships remained significant when the authors averaged the ratios of the left and right hand and the drive for muscularity finding remained significant when the authors used the right hand as the predictor.
A lower 2D:4D ratio also predicted lower levels of eating disordered behaviors in men. The relationship only approached statistical significant (p = .09) when gay men were included in the sample and the results were not significant when the average of both hands or the right hand were used as the predictor.
So, what do these findings tell us? First of all, it appears that, for men as with women, a greater level of prenatal testosterone is associated with less of a drive to be thin and lower levels of eating disordered behaviors. Additionally, a greater level of prenatal testosterone exposure appears to predict a greater drive to develop a muscular physique.
Admittedly, when I first heard about the use of digit ratios in psychopathology research, I was skeptical. In fact, several years ago I had an opportunity to review a paper that involved digit ratios, but declined because I had not heard of this phenomenon and was entirely surprised by it. Having now had the opportunity to read more about this phenomenon and to collect data on it myself, I am a firm believer in its utility, even if it is an imperfect measure of prenatal testosterone exposure. Certainly better methods exist, but the digit ratio offers an easy and useful tool for considering biological risks.
Importantly, keep in mind that the authors are not attempting to say that eating disorders are entirely biologically determined. They are simply attempting to clarify one of the ways in which a particular biological marker might be used to predict vulnerability to eating disordered beliefs and behaviors. Quite obviously, there is nothing we can do after the fact to adjust how much testosterone an individual was exposed to in utero, so this is not a target for therapeutic interventions; however, understanding this relationship can help clarify one of the ways in which our own body makes us more or less vulnerable to particular outcomes and can help us predict risk well before the onset of symptoms and potentially utilize preventative care for vulnerable individuals.
Future research using clinical samples and comparing both male and female participants simultaneously would be highly useful, but the authors did a great job of supplementing the current literature and providing a foundation for future examinations of biological predictors of eating disorders in males.
If you would like to learn more about eating disorders, we recommend the following resources, all of which are available through our online store:
- Overcoming Binge Eating
 by Christopher Fairburn
by Christopher Fairburn
-
Crave: Why You Binge Eat and How to Stop
 by Cynthia Bulik
by Cynthia Bulik
-
Dialectical Behavior Therapy for Binge Eating and Bulimia
 by Debra Safer, Cristy Telch, and Eunice Chen
by Debra Safer, Cristy Telch, and Eunice Chen
- Overcoming Your Eating Disorder: A Cognitive-Behavioral Therapy Approach for Bulimia Nervosa and Binge-Eating Disorder, Guided Self Help Workbook
 by Stewart Agras and Robin Apple
by Stewart Agras and Robin Apple
- Treatment Manual for Anorexia Nervosa: A Family-Based Approach
 by James Lock, Daniel le Grange, and Stewart Agras
by James Lock, Daniel le Grange, and Stewart Agras
- Eating with Your Anorexic: How My Child Recovered Through Family-Based Treatment and Yours Can Too
 by Laura Collins
by Laura Collins
Mike Anestis is a doctoral candidate in the clinical psychology department at Florida State University


 Subscribe in a reader
Subscribe in a reader


